

Generalised Anxiety Disorder (GAD)
Children with GAD experience excessive anxiety and worry about multiple events and/or activities. They find it difficult to control these feelings and this can interfere with their ability to pay attention to or complete tasks. The probability of a negative outcome is overestimated and excessive for the situation, and the experience of symptoms significantly impacts everyday functioning.
What does GAD look like?
- Restlessness/feeling on edge
- Excessive anxiety and apprehension with future events
- Becomes tired easily
- Difficulty with concentrating
- Irritable
- Difficulty sleeping (falling asleep, staying asleep, and/or quality of sleep)
- Muscle tension
- Other physical experiences, including increased heart rate, shortness of breath, sweating, nausea, and/or diarrhea.


Source: @what.is.mental.illness, 'Generalised Anxiety Disorder'

Source: @theburntoutbrain, 'Anxiety Be Like'
The contextual factors that drive stress/distress, or perceived threats, occur at much higher levels for Autistics.
Some examples of why this is:
- Intolerance of uncertainty
- Repetitive thinking style and perfectionist traits
- A sense that others see them as ‘less' than, ‘defective’ or ‘not acceptable’
- Autistic masking's physical and emotional demands
- Sensory stress/distress
- Self-calming activities/actions may not be available or not allowed
Obsessive Compulsive Disorder (OCD)
Obsessive-compulsive disorder (OCD) features a pattern of unwanted thoughts and fears (obsessions) that lead you to do repetitive behaviours (compulsions). These obsessions and compulsions interfere with daily activities and cause significant distress.
You may try to ignore or stop your obsessions, but that only increases your distress and anxiety. Ultimately, you feel driven to perform compulsive acts to try to ease your stress. Despite efforts to ignore or get rid of bothersome thoughts or urges, they keep coming back. This leads to more ritualistic behaviour - the vicious cycle of OCD.
OCD often centres around certain themes - for example, an excessive fear of getting contaminated by germs. To ease your contamination fears, you may compulsively wash your hands until they're sore and chapped.
If you have OCD, you may be ashamed and embarrassed about the condition, but treatment can be effective.
Obsessive-compulsive disorder usually includes both obsessions and compulsions. But it's also possible to have only obsession symptoms or only compulsion symptoms. You may or may not realize that your obsessions and compulsions are excessive or unreasonable, but they take up a great deal of time and interfere with your daily routine and social, school or work functioning.
OCD obsessions are repeated, persistent and unwanted thoughts, urges or images that are intrusive and cause distress or anxiety. You might try to ignore them or get rid of them by performing a compulsive behaviour or ritual. These obsessions typically intrude when you're trying to think of or do other things.
Obsessions often have themes to them, such as:
- Fear of contamination or dirt
- Doubting and having difficulty tolerating uncertainty
- Needing things orderly and symmetrical
- Aggressive or horrific thoughts about losing control and harming yourself or others
- Unwanted thoughts, including aggression, or sexual or religious subjects
Examples of obsession signs and symptoms include:
- Fear of being contaminated by touching objects others have touched
- Doubts that you've locked the door or turned off the stove
- Intense stress when objects aren't orderly or facing a certain way
- Images of driving your car into a crowd of people
- Thoughts about shouting obscenities or acting inappropriately in public
- Unpleasant sexual images
- Avoidance of situations that can trigger obsessions, such as shaking hands
OCD compulsions are repetitive behaviours that you feel driven to perform. These repetitive behaviours or mental acts are meant to reduce anxiety related to your obsessions or prevent something bad from happening. However, engaging in the compulsions brings no pleasure and may offer only a temporary relief from anxiety.
You may make up rules or rituals to follow that help control your anxiety when you're having obsessive thoughts. These compulsions are excessive and often are not realistically related to the problem they're intended to fix.
As with obsessions, compulsions typically have themes, such as:
- Washing and cleaning
- Checking
- Counting
- Orderliness
- Following a strict routine
- Demanding reassurance
Examples of compulsion signs and symptoms include:
- Hand-washing until your skin becomes raw
- Checking doors repeatedly to make sure they're locked
- Checking the stove repeatedly to make sure it's off
- Counting in certain patterns
- Silently repeating a prayer, word or phrase
- Arranging your canned goods to face the same way

Source: @ocddoodles, 'OCD'

Source: @ocdexcellence, 'How OCD Feels'

Source: @ocddoodles, 'The OCD Cycle'
OCD usually begins in the teen or young adult years, but it can start in childhood. Symptoms usually begin gradually and tend to vary in severity throughout life. The types of obsessions and compulsions you experience can also change over time.
Symptoms generally worsen when you experience greater stress. OCD, usually considered a lifelong disorder, can have mild to moderate symptoms or be so severe and time-consuming that it becomes disabling. If you have OCD, you may be ashamed and embarrassed about the condition, but treatment can be effective.
The Severity of OCD
The cause of obsessive-compulsive disorder isn't fully understood. Main theories include:
- Biology - OCD may be a result of changes in your body's own natural chemistry or brain functions.
- Genetics - OCD may have a genetic component, but specific genes have yet to be identified.
- Learning - Obsessive fears and compulsive behaviours can be learned from watching family members or gradually learned over time.
Factors that may increase the risk of developing or triggering obsessive-compulsive disorder include:
- Family history - Having parents or other family members with the disorder can increase your risk of developing OCD.
- Stressful life events - If you've experienced traumatic or stressful events, your risk may increase. This reaction may, for some reason, trigger the intrusive thoughts, rituals and emotional distress characteristic of OCD.
- Other mental health disorders - OCD may be related to other mental health disorders, such as anxiety disorders, depression, substance abuse or tic disorders.

Pathological Demand Avoidance (PDA)
Pathological demand avoidance (PDA) is a proposed subtype of Autism Spectrum Disorder but is not yet recognised by the DSM-5 and may be unlikely to be given the umbrella diagnosis of 'ASD' has been adopted (and removed Asperger’s Syndrome).
PDA is a very new and not well-recognised condition in the field which makes diagnosis and support even more challenging.

Source: @autieselfcare, 'The PDA Profile'
Those with a demand avoidant profile share difficulties with others on the Autism Spectrum in social communication, social interaction and restricted and repetitive patterns of behaviours, activities or interests. However, those who present with this particular diagnostic profile are driven to avoid everyday demands and expectations to an extreme extent.
It may appear as though someone with PDA has better social understanding and communication skills than others on the Autism Spectrum and are able to often use this to their advantage. Although children with PDA seem to socialise well, have fair eye contact, and are able to mask their weaknesses pretty well on the surface, their underlying social skills and ability to read social situations are poor, as more recent research into this condition has determined.
The demand avoidant behaviour is rooted in an anxiety-based need to be in control as research has shown that underneath the strong social façade and pretence is a person who feels very inadequate, scared, and insecure. The anxiety and fear control every aspect of their daily life. The need to control everything, following nothing, and avoid all daily demands is driven by this anxiety and strong feelings of inferiority.
Life becomes too scary and overwhelming that they often mix reality with fantasy to create a world that they feel safe and competent. This usually means refusing to follow anyone else’s guidance, since to do so leaves them vulnerable to uncertainty and increased anxiety. This is not just common anxiety, but a deep-rooted fear.
Those with PDA often make up elaborate reasons to avoid requests, demands and any expectations (they are sick, too smart for something that stupid, will do it later, redirect peoples attention elsewhere, etc.) They even find it hard to meet their own desires and expectations., eventually withdrawing into a defensive mode of avoiding all meaningful life activities that parents and others try to coax or demand them into doing.
Unfortunately, most adults (parents, teachers, professionals) view them as defiant, manipulative, and purposely oppositional, which only fuels their need to command and demand even more.
- Resists and avoids the ordinary demands of life
- Uses social strategies as part of avoidance, e.g. distracting, giving excuses
- Appears sociable, but lacks understanding
- Experiences excessive mood swings and impulsivity
- Appears comfortable in role play and pretence
- Displays obsessive behaviour that is often focused on other people.
People with this profile can appear controlling and dominating, especially when they feel anxious. However, they can also be enigmatic and charming when they feel secure and in control.
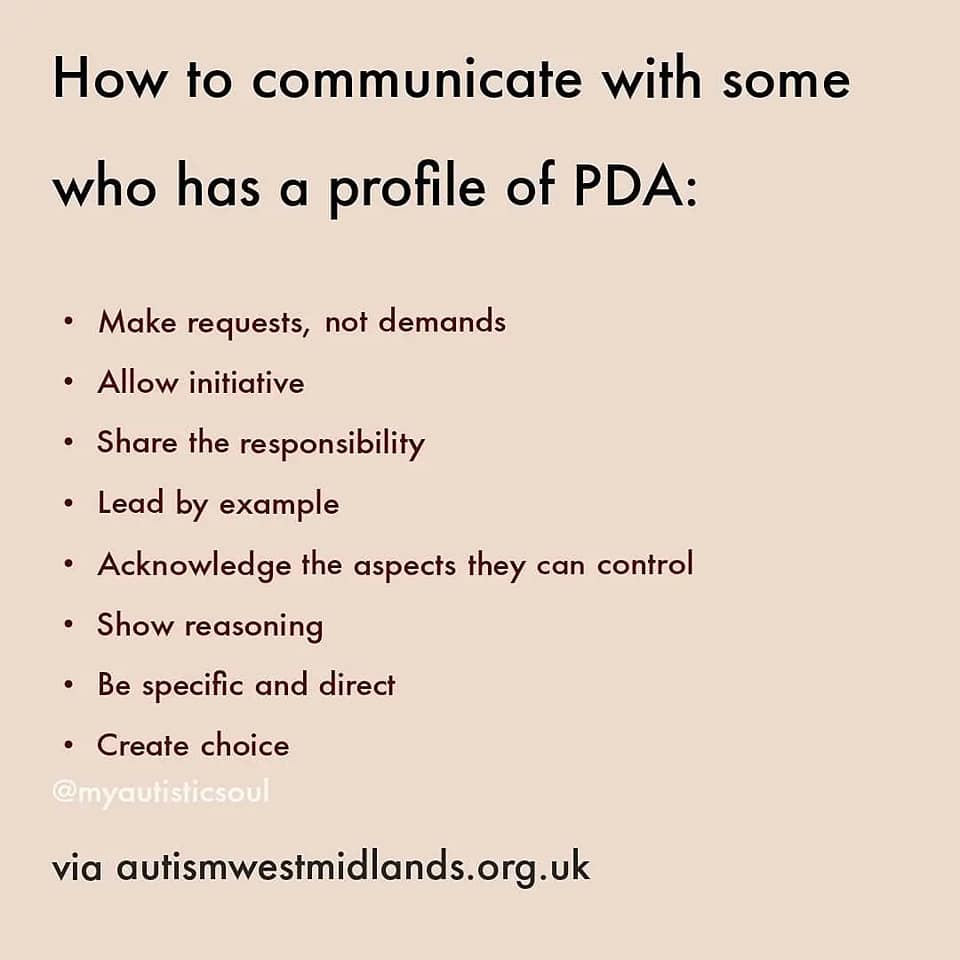
Supporting those with PDA is extremely challenging, as they can too easily become more resistant and sophisticated in their avoidance, sabotage everything that looks like external control, even refuse to do what they like if others are requesting it. Pressure only pushes them further into being defiant and not trusting the guidance of others. Only by backing off the demands, letting them control and trust that you will let them, and gradually building a collaborated relationship with them, can you lessen the anxiety and build more trust in your guidance.
Children with PDA are the most complex and vulnerable children to help. They resist almost every parenting, teaching, and disciplinary technique common to children. The harder you try to help (by instructing, directing, prompting, etc.) the more they resist, the more they act out and the further away they become from feeling safe with others. Very frustrating and heartbreaking for parents and teachers.
When you try to reverse your strategies to a low-demand, collaborative, working partnership model, you are chastised by other parents, family, teachers, and professionals.


Oppositional Defiance Disorder (ODD)
ODD is a pattern of behaviours characterised by angry/irritable mood, argumentative/defiant behaviour and vindictiveness. These difficulties can result in conflict with teachers, parents and peers which can lead to issues with children’s emotional and social development as well as academic performance. ODD is somewhat more common in pre-adolescent boys compared to girls.
In order to tell the difference between typical disruptive behaviour and ODD is to examine how severe the behaviour is and how long it lasts and for ODD to be diagnosed, the behaviour must last at least six months and involve at least one person who isn’t a sibling.
ODD is often mistaken for ADHD, so careful observation by practitioners over a period of time is highly recommended.
What does ODD look like?
- Angry mood – frequent and easy loss of temper
- Annoyance, touchiness, and resentfulness
- Arguing with authority figures/adults
- Actively defying or refusing to follow instructions or rules
- Deliberately annoying others
- Blaming others for mistakes or misbehaviour
- Being spiteful or vindictive

Source: @mightier

Source: @mollyadhd, Adapted from 'ADHD & ODD'

Source: @mollyadhd, Adapted from 'ADHD & ODD'